This past Friday I was back in DC for a meeting of policy thinkers, analysts and researchers interested in obtaining a better understanding of how the Affordable Care Act affects the nation’s public health system. This is a complicated question to answer for many reasons. To name just a few: First, responsibility for financing and implementing public health programs and policies has long been an intergovernmental and multi-organizational enterprise in the U.S. Teasing out the effects of law and policy implementation on a “system” with so many semi-autonomous actors and actions is a daunting task. Second, the protracted effects of the 2008 economic recession has co-occurred with ACA adoption and implementation, making it difficult to untangle the effects. Reductions in state, local, and federal government spending for public health activities have occurred over the past five years. Other confounding developments during this period include the development of a national voluntary accreditation program for state and local public health agencies (PHAB), and the adoption of numerous state and local laws designed to reform the organization and financing of public health services.
Third, the ACA has many moving parts that are likely to vary in their magnitude, timing, and distribution of impact on population health and cost containment goals. Some changes in public health delivery are mobilized directly by new federally-funded initiatives supported through the Prevention and Public Health Fund, such as the Community Transformation Grant Program and the National Public Health Improvement Initiative. Other changes are occurring through indirect routes, as state and local governments recalibrate what public health programs and services to support and how to finance these activities, based on current and anticipated changes in health insurance coverage (e.g. mandated first-dollar coverage for clinical preventive services, and expansions in health insurance coverage through Medicaid the insurance exchanges). Still other public health system changes are occurring as a result of efforts to redesign medical care delivery and financing mechanisms through ACA initiatives such as the CMS Innovation Center initiatives, the new IRS community benefit requirements for tax-exempt hospitals, and new incentives for insurers and employers to invest in health promotion and disease prevention activities. These efforts are leading some public health agencies to renegotiate their responsibilities and relationships with health care system stakeholders.
Although considerable policy attention has focused on the Prevention Fund, the indirect effects of ACA on public health systems have the potential to be particularly large and far-reaching. For example, a 2012 Institute of Medicine report noted that state and local governments have the potential to strengthen core public health programming substantially under ACA by adopting the following recommendation:
“Recommendation 9: The committee recommends that state and local public health funding currently used to pay for clinical care that becomes reimbursable by Medicaid or state health insurance exchanges under Affordable Care Act provisions be reallocated by state and local governments to population-based prevention and health promotion activities conducted by the public health department.”
However, anecdotal evidence suggests that some governments (for example, Kentucky) are considering alternative actions that involve redirecting state and local funding from core public health activities in order to support the implementation of more immediate needs related to health insurance expansion and medical care delivery system reform. A broader and more systematic understanding of how the nation’s public health system is changing in response to the ACA is needed to inform policy and administrative mechanisms for improving population health and achieving efficient resource use at all levels within the system.
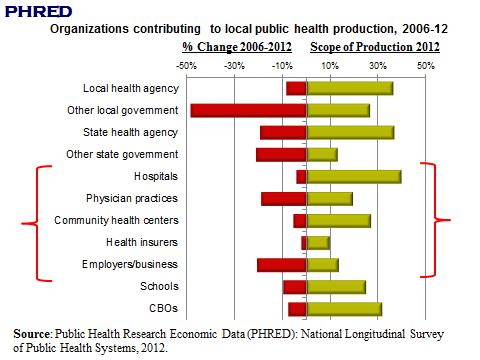
What evidence do we have so far? Some of my own recent research shows that the combined effects of the economic recession and the early phases of ACA implementation have triggered some important changes in the production of public health activities at the community level in recent years (Figure above). The National Longitudinal Survey of Public Health Systems allows us to monitor about 360 metropolitan communities over time (since 1998), tracking which public health activities are available in each community, which agencies and organizations contribute to each one, and how well these activities are performed as assessed by the local public health official. As the figure shows, state and local government agencies, along with community hospitals, tend to contribute to the broadest scope of public health activities in the average metropolitan community. All of the organizations that we monitor reduced the number of public health activities that they support between 2006 and 2012 – a response that is attributable primarily to recessionary contraction (we show this analytically in a forthcoming paper and in work presented at APHA last month).
However, some of the organizations contributing to public health activities appear more resistant to recessionary contraction than others. In particular, some of the health care delivery and financing organizations that face new ACA incentives for engaging in public health and prevention activities (shown in brackets in the figure above) were fairly successful in preserving their public health contributions during the 2006-12 period. How much of this trend is attributable to ACA provisions and incentives remains to be sorted out, and will require additional data to be collected over the next few years of ACA implementation.
On a related note, earlier this year we completed some preliminary analyses that examine the extent to which private-sector organizations complement vs. substitute for the work of governmental public health agencies when they contribute to public health activities. The early results suggest a mixed bag, with hospital contributions being primarily complementary while the contributions of physician practices and employers function as substitutes.
With the most far-reaching components of ACA scheduled for implementation beginning next month, these early results must be interpreted with caution. The need for high-quality research on public health delivery and impact has perhaps never been greater – hence the reason for my DC meeting on Friday. To facilitate economic-related research on public health delivery, we will soon launch a new electronic resource called Public Health Research Economic Data (PHRED) that can serve as an inventory of publicly accessible data sources and measures useful for such studies – some of which are being developed through the work of our Public Health PBRN program. (The homophony with the Federal Reserve’s wonderful data repository FRED is mostly coincidental). Stay tuned to this blog and our PHSSR website for more information on PHRED and on progress with estimating the effects of ACA on the nation’s public health system.

Pingback: Research and Public Health Innovation | Public Health Economics
Pingback: Understanding the Joint Production of Public Health and Personal Health Services | Public Health Economics
Pingback: Next Generation Public Health: Can Laboratories Enhance the Value Stream? | APHL Public Health LabLog
Pingback: Better Living through Chemicals? Addressing Substitution Effects in Medicine and Public Health | Public Health Economics