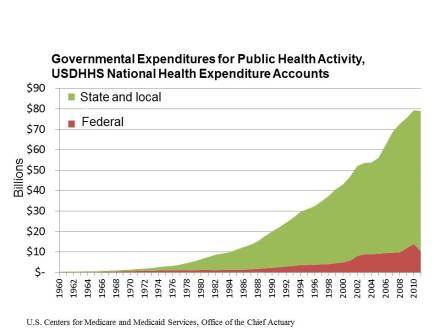
I use this slide in my lectures frequently and I am always surprised at how many career public health professionals express shock and disbelief at this fundamental financial truth: the federal government is a small minority investor in the U.S. public health enterprise. Of the nearly $80 billion in governmental spending on public health activity in the U.S., the federal government accounts for only about 15% of the outlays. States and especially local governments provide the lion’s share of the resources that keep public health programs and policies operational around the country. To be sure, we can quibble with the quality of the data collected by the Census Bureau on governmental public health expenditures, but the basic levels and trends can’t be too far off.
One of the important implications of this 15% is that, by pure mathematics, it is impossible for the federal government to be very effective in smoothing out imbalances that exist between public health needs and public health resources across states and communities. State and local governments depend heavily on revenue sources like income taxes, sales taxes, and property taxes to finance their activities. As a result, public health spending tends to reflect the underlying inequalities in household income and housing wealth that exist across the U.S. Poorer communities face higher levels of preventable disease burden and health risks, and yet they have less fiscal capacity to invest in the strategies that could reduce this burden. And of course, these financing mechanisms mean that public health spending tends to be highly unstable over time and sensitive to macroeconomic events like recessions that influence employment, earnings, consumption, and housing prices.
Prior to the 1960s, very similar patterns held true for medical care spending. But since that time, the federal government has stepped in to play a much larger role in financing medical care through programs like Medicare, Medicaid, and SCHIP. To be sure, there is still considerable variation in medical care spending per person across states and localities, but these patterns of variation no longer track so tightly with socioeconomic status.
But for now, where you live continues to determine the level of public health protections that you enjoy. There will be more empirical work on this topic to discuss at the upcoming American Public Health Association Annual Meeting in Boston starting this weekend, so stay tuned.

Pingback: No Recovery Yet in Public Health Spending | Public Health Economics